The average FHIR API implementation takes somewhere between four and six months. Teams spend weeks in discovery, months mapping legacy HL7 v2 data to FHIR resources, and then more time retrofitting authentication and fixing conformance issues that a validator surfaces at the end. By the time they go live, the original deadline has passed, and the engineering team is exhausted.
It does not have to work that way. The underlying technology now enables rapid delivery. FHIR’s RESTful architecture means that, with the right setup, developers can build functional APIs in a fraction of the time that HL7 v2 integrations once required. The gap between what is possible and what most teams experience comes down to four architectural decisions made at the start of the project, not the end.
This guide walks through those decisions, a realistic six-week delivery timeline, and the common traps that add months to projects that should ship in weeks.
Why Most FHIR Projects Take Longer Than They Should
The healthcare industry is in the middle of a regulatory push that has made FHIR non-negotiable. The ONC’s HTI-1 Final Rule required USCDI v3 support via FHIR APIs by January 1, 2027, and the CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) mandates FHIR-based prior authorization APIs for payers by January 2027. Meanwhile, global adoption is accelerating; the 2025 State of FHIR Survey found that 73% of countries now explicitly mandate or recommend FHIR usage, up from 56% just two years ago.
The pressure is real. But pressure does not explain why projects run long. The real reasons are usually one of three things.
Scope Creep at the Requirements Stage
The most common cause of timeline inflation is attempting to implement every FHIR resource the team can think of before writing a single line of code. A fully featured FHIR R4 implementation has 145 defined resources. For most HIT vendor projects, a compliant and useful v1 requires five to eight. Teams that do not enforce a minimum resource set at the start spend weeks mapping, validating, and testing resources that no consumer has yet asked for.
The fix is discipline, not technology. Define your minimum resource set: Patient, Encounter, Observation, Condition, and Practitioner cover the majority of ONC-required patient access use cases, and lock it before development begins.
Choosing the Wrong FHIR Server
Teams that decide to build a custom FHIR server from scratch because it “gives us more control” routinely add two to three months to a project. Mature, pre-validated FHIR servers already exist, Azure API for FHIR, AWS Health Lake, Google Cloud Healthcare API, and the open-source HAPI FHIR server all support FHIR R4, SMART on FHIR, and HIPAA-compliant data storage. Choosing one of these instead of building from scratch eliminates the provisioning and certification overhead entirely.
The server selection decision is the single highest-leverage choice in a FHIR project. Make it in week one.
Underestimating the Data Mapping Work
Most HIT vendors have years of patient data stored in HL7 v2 message formats, ADT feeds, ORU results, and ORM orders. That data needs to be transformed into FHIR-compliant JSON before it can be served through a FHIR API. Teams that build this transformation directly into their application code create a brittle, hard-to-maintain layer. Teams that build a dedicated translation layer using a mature integration engine, Mirth Connect, Azure Logic Apps, BizTalk, keep the transformation isolated and testable.
Data mapping is not a task that can be compressed. But it can be parallelized. Running the translation layer build alongside the FHIR server setup, rather than sequentially, typically saves two to three weeks on its own.
64% of US outpatient settings were using FHIR app access in 2024, up from 49% in 2021. FHIR is now mainstream — the vendors who have not implemented it are already behind.
Source: ONC / Aptarro EHR Adoption Report, 2024
The Four Architecture Decisions That Define Your Timeline
Speed comes from making the right decisions early, not from moving faster. Here are the four choices that determine whether a FHIR project ships in six weeks or six months.
Decision 1: Choose a Managed FHIR Server
Comparing the main options on two axes, time to first working endpoint, and ongoing maintenance overhead, managed cloud options win on both for most teams. Azure API for FHIR can be provisioned and configured in hours, not weeks. It ships with built-in HIPAA controls, OAuth2 support, and SMART on FHIR compatibility out of the box. HAPI FHIR is a strong open-source alternative for teams that need self-hosted control, but it requires more infrastructure setup.
The question is not which server is technically superior. The question is which one gets you to a working endpoint fastest, given your team’s existing cloud expertise. For most US healthcare vendors on Azure infrastructure, Azure API for FHIR is the straightforward answer. For teams on AWS, AWS HealthLake is the equivalent.
Decision 2: Define Your Minimum Resource Set
Before any development starts, produce a list of the FHIR resources your API must support for v1. For ONC Patient Access API compliance, the baseline covers: Patient, Allergy Intolerance, Care Plan, Care Team, Condition, Device, Diagnostic Report, Document Reference, Encounter, Goal, Immunization, Medication Request, Observation, Procedure, and Provenance. However, most vendors do not need all of these for their initial deployment; a minimum viable set of five to seven resources covers the high-priority use cases and dramatically reduces the mapping and testing scope.
Document the scope in writing, get sign-off from product and engineering, and resist the temptation to add resources until v1 is live.
Decision 3: Build a Dedicated Translation Layer
Your FHIR API’s job is to serve FHIR-formatted data. It should also not be responsible for transforming messy, inconsistently formatted source data. A dedicated translation layer, typically an integration engine sitting between your source systems and the FHIR server, handles the HL7 v2-to-FHIR mapping, data normalization, and error handling independently of the API itself.
Mirth Connect is the most widely used open-source option in healthcare. Azure Logic Apps and BizTalk are strong choices for teams already in the Azure ecosystem. The investment in building this layer pays back immediately in testing speed and maintainability. When a partner changes their HL7 feed format, only the translation layer needs updating, not the API.
Decision 4: Design SMART on FHIR Authentication from Day One
SMART on FHIR (which stands for Substitutable Medical Applications, Reusable Technologies) is the authorization framework for FHIR APIs: it defines how third-party apps authenticate and what data they can access. It is based on OAuth2 and is required for ONC Patient Access API compliance.
Teams that treat authentication as something to configure after the API is built routinely add two weeks to a project. The SMART on FHIR scopes, the OAuth2 authorization server configuration, and the token handling logic need to be designed into the architecture from week one, not bolted on in week five.
A Realistic Six-Week FHIR API Delivery Timeline
The following timeline assumes a team of three to four engineers, a defined minimum resource set, a managed FHIR server selection made before kickoff, and source data available in HL7 v2 or structured flat files.
| Week 1 | Discovery and scoping: Map source data fields to FHIR resource attributes. Confirm minimum resource set. Select and provision a FHIR server. Configure SMART on FHIR OAuth2 framework. |
| Week 2 | Environment setup: FHIR server configured and accessible. SMART on FHIR auth flows tested in sandbox. Integration engine (Mirth/Logic Apps) set up with source system connections. |
| Week 3 | Data mapping: Build translation logic for each resource. Map HL7 v2 segments to FHIR JSON attributes. Handle edge cases in source data: missing fields, non-standard codes, and local value sets. |
| Week 4 | API development: Build CRUD endpoints (GET, POST, PUT, search) for each resource. Unit test each endpoint against the FHIR R4 specification. Fix mapping issues surfaced during testing. |
| Week 5 | Integration testing: End-to-end tests with real source data. SMART on FHIR auth flow testing with consumer apps. Performance testing for expected query volumes. |
| Week 6 | Validation and go-live: Run the ONC’s Inferno FHIR validator against all endpoints. Fix any conformance issues. Security review. Staged production deployment. Monitoring and alerting are configured. |
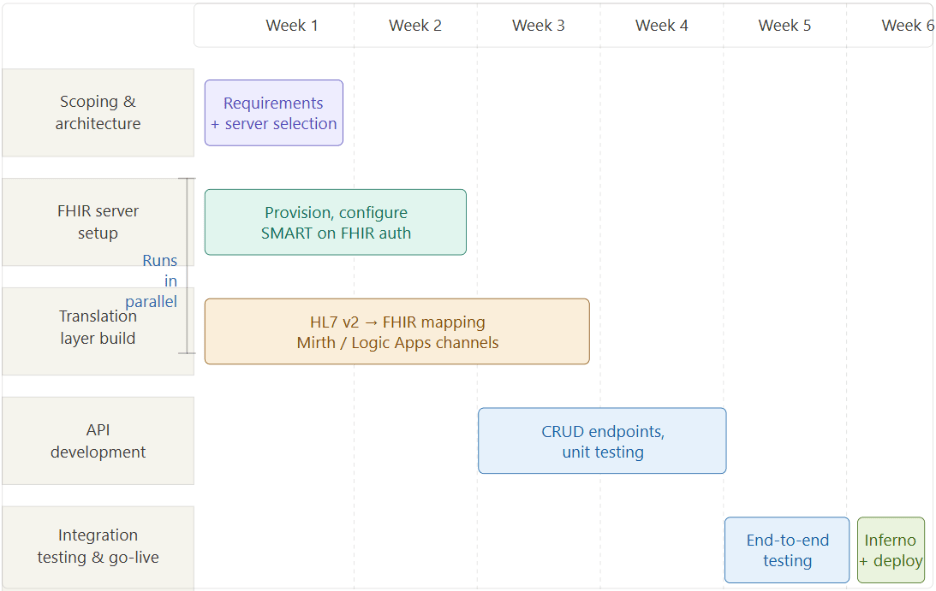
The week-by-week schedule above describes what happens in sequence. What it doesn’t fully show is what should run in parallel. Most delays come from treating server setup and translation layer build as sequential, finishing one, then starting the other. The diagram below shows the parallel track model that compresses delivery:
Real Example: A Fertility EMR Cuts Integration Time from Weeks to Days
One of the clearest illustrations of what this approach delivers at scale comes from Nalashaa’s engagement with a leading fertility EMR provider serving more than 32% of fertility practices in the United States, more than 120 clinics. The client’s existing integration architecture required at least one month of work per vendor integration, at a cost of approximately $30,000 each. Scaling this across 120+ clinics was unsustainable.
Nalashaa’s approach was to deploy an Azure FHIR server as a centralized data hub, with a multi-tenancy setup allowing clinics and vendors to query the server after authentication via a cloud IAM layer. An Enterprise Service Bus framework handled message routing and asynchronous communication across integration channels. In four months, a team of four engineers completed a setup that the client estimated would have taken twelve months or more to build internally.
The result: integration time per vendor dropped from four weeks to under one week for multiple parallel integrations. The client saved an estimated $240,000 in infrastructure build costs. And the FHIR hub opened a new monetization channel: the client now earns revenue for every new patient record registered in the vendor system.
Nalashaa’s fertility EMR project: integration time per vendor reduced from 4 weeks to under 1 week. Total savings: $240,000. Build time: 4 months vs. estimated 12+ months.
Three Questions to Answer Before You Write a Single Line of Code
If you are scoping a FHIR API project right now, these three questions determine more about your timeline than anything else.
- What is your minimum viable resource set for v1? Write it down and get a sign-off. If anyone adds a resource after this point, it requires a formal scope change.
- Does your source data exist in a structured format, HL7 v2, flat files, a relational database, or will you need to extract and clean it first? Unstructured or inconsistently formatted source data adds two to four weeks, which has nothing to do with FHIR.
- Which FHIR server option best fits your compliance requirements, hosting preferences, and team’s existing cloud expertise? Make this decision in week one, not after discovery.
These are not rhetorical questions. Teams that cannot answer all three before starting development almost always hit the same delays, scope expansion, server rework, and auth issues in the final week. A thirty-minute scoping call with a FHIR implementation partner can resolve all three.
The Path Forward
The regulatory timeline for FHIR is not slowing down. The CMS Prior Authorization API rule requires payer-facing FHIR APIs to be fully compliant by January 2027. The HTI-1 mandate is already in effect. The 2025 State of FHIR Survey found that 84% of healthcare leaders expect FHIR adoption to grow steadily, and the healthcare interoperability market is projected to more than triple from $3.97 billion in 2024 to $13.60 billion by 2034.
Building a FHIR API in weeks rather than months is not about cutting corners. It is about making four right decisions at the start of the project instead of learning from four wrong ones halfway through. Start narrow. Choose a managed server. Build a translation layer. Design auth from day one.
If your team is scoping a FHIR project right now and the timeline feels longer than it should, it is usually one of those four decisions.
READY TO TAKE THE NEXT STEP?
Nalashaa’s interoperability team has delivered FHIR integrations for EHR vendors, fertility platforms, behavioral health providers, and payers across the US healthcare market. If your FHIR project timeline is longer than six weeks, let’s talk about what’s driving it. A 45-minute call is usually enough to diagnose the bottleneck.
→ Book a Free FHIR Integration Assessment or connect with us at info@nalashaa.com
Frequently Asked Questions
Q: How long does FHIR API development take?
A: With the right architecture and a defined minimum resource set, a production-ready FHIR R4 API can be delivered in 6 weeks. Industry benchmarks show 63% of developers now build functional FHIR APIs in under one week. The typical 4–6 month timeline reflects scope creep, wrong tooling choices, and retrofitted auth — not the inherent complexity of the standard.
Q: What FHIR server should I use?
A: For most US healthcare vendors, a managed cloud option — Azure API for FHIR, AWS Health Lakee, or Google Cloud Healthcare API- is faster to deploy and easier to maintain than a self-hosted HAPI FHIR instance. The right choice depends on your existing cloud infrastructure and compliance requirements.
Q: What is SMART on FHIR?
A: SMART on FHIR is the OAuth2-based authorization framework for FHIR APIs. It defines how third-party apps authenticate and what data they can access. It is required for ONC Patient Access API compliance and must be designed into the architecture from the start of a project.
Q: What is the minimum FHIR resource set?
A: A minimum resource set is the specific list of FHIR resources your API will support in its first version. For ONC Patient Access compliance, the most common minimum set includes Patient, Encounter, Observation, Condition, and Practitioner. Defining this scope before development starts is the single most effective way to control the timeline.
Q: How much does FHIR API implementation cost?
A: Cost varies significantly based on team size, source data complexity, and server choice. A managed Azure FHIR server with a dedicated translation layer and a three-person engineering team can be delivered in 6 weeks at significantly lower cost than a custom-built solution. Nalashaa’s fertility EMR case shows a $240,000 saving versus a self-build estimate.
Latest posts by Priti Prabha (see all)
- How to Build a FHIR API in Weeks, Not Months - April 13, 2026