After-hours documentation has become one of the defining frustrations of US clinical practice, the reason a physician’s working day so often ends well after the last patient has left. Ambient AI scribes, which listen to a visit and generate a draft note from the conversation, are the most credible response the industry has produced to that burden, and over the past two years, they have moved out of pilot projects and into routine use. Epic now ships its own ambient scribe; athenahealth began offering one to its customers at no charge in early 2026, and a substantial share of hospitals running Epic have already enabled ambient documentation in some form.
Acquiring one, then, has become the straightforward step. What separates a deployment that genuinely lowers burnout from one that ends up as an expensive contract nobody opens is the work that no purchase order describes: keeping the patient audio within HIPAA, returning the finished note to the EHR in a form clinicians can rely on, and persuading those clinicians to fold the tool into the way they already work. This guide is about those three problems, and it is written for the health systems, clinics, and HIT vendors that must solve them rather than for the buyers choosing between products.
What Research Shows About Ambient AI Scribes
The research that exists points in a reasonably consistent direction. A 2025 randomized trial at UCLA Health that set two ambient scribes against usual care found what most of the literature now echoes: ambient documentation reduces the time clinicians spend writing notes and, more dependably, eases burnout. UW Health recovered close to half an hour per provider each day in its own trial and extended the system to hundreds of clinicians afterward.
Those same studies carry a qualification that vendor presentations tend to leave out. Where documentation time falls, it falls unevenly, and across most settings, the total length of a visit and the number of patients seen in a day barely move. An ambient scribe will not let a clinic run more appointments, and its real dividend arrives as fewer hours of evening charting, lower burnout, and more attention on the patient during the encounter. A business case built on throughput will disappoint the people who approved it, whereas one built on retention, wellbeing, and the quality of the record will hold up under review. Because that distinction governs how the entire rollout is later judged, it is worth settling what you intend to measure before the first clinician is brought on.
HIPAA, Patient Consent, and Clinical Documentation Requirements
As soon as an ambient scribe begins listening, a new flow of protected health information comes into being. The audio of the encounter and the transcript drawn from it are ePHI, and the vendor that processes them is a business associate under HIPAA, which makes a Business Associate Agreement necessary without making it anywhere near sufficient on its own.
An agreement drafted for a storage provider will not address what an AI vendor does with the data. It has to speak to the processing pipeline itself: whether your audio may be used to train the vendor’s models, how subcontractors are governed, how long audio and transcripts persist, what becomes of your data when the relationship ends, and what audit rights you retain over all of it. Retention varies widely, with some vendors deleting audio after roughly thirty days and others keeping it indefinitely unless you intervene, so that detail belongs in the procurement conversation rather than in a later post-incident review.
Consent is where organizations are being caught at the moment. HIPAA on its own does not require special patient consent to document a treatment encounter, but state law frequently does. In all-party-consent states, recording a conversation without informing the patient can collide with wiretapping statutes, a risk that turned concrete in late 2025 when a proposed class action against a California health system alleged that around 100,000 visits had been recorded without adequate consent, with comparable suits appearing elsewhere soon after. A spoken disclosure at the start of the visit, a corresponding line in the Notice of Privacy Practices, and a straightforward way for a patient to decline together cost very little against the scale of that exposure.
Two further controls belong in the design from the beginning. Introducing an ambient scribe rewrites the data map, so it should prompt a refresh of the security risk analysis, the access controls, and the incident response plan. The clinician also has to remain the author of record, because these models can fabricate a detail or drop something that was said, and a review-and-attestation step before the note reaches the chart is the safeguard that keeps an AI draft from entering the record as an unreviewed legal document.
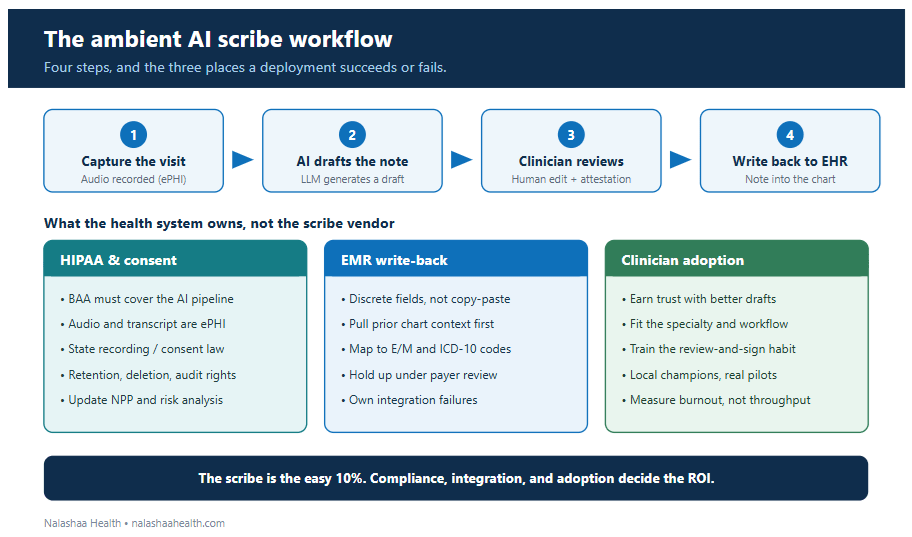
Figure: Capture, draft, review, and write-back, with the make-or-break checkpoints at each stage. The scribe handles the middle; the compliance, integration, and adoption work is what a health system owns.
EMR Write-Back and EHR Integration Requirements
Recording a conversation and producing a draft is the portion of the workflow that performs well in a demonstration. Returning that draft to the EHR correctly is the portion that determines whether clinicians keep the tool, and it is where most of the engineering effort actually lives.
A meaningful distance separates a scribe that places finished text into the correct discrete chart fields from one that leaves the clinician copying out of a side panel and pasting into the record. Pasting is tolerable in a demonstration and becomes a daily irritation once a physician is repeating it across a full schedule. Write-back done properly means the note arrives in the right encounter and the right fields, draws on the prior chart, the medication list, and the problem list before the visit, so the draft begins informed rather than empty, and resolves into the structured data that the surrounding systems depend on.
Coding is the point at which write-back meets compliance, and it deserves separate thought. Analyses through 2025 observed evaluation-and-management coding drifting upward after ambient scribes were adopted, and at least one large payer responded by routing more of the higher-level E/M claims into automatic review. A scribe that produces fuller notes can shift a billing profile without anyone intending it to, so the documentation has to survive payer scrutiny rather than simply read well. Building that integration, mapping the output to codes, identifying the encounters where it breaks, and owning the path to resolution is the work a scribe vendor will hand back to your EHR team. Enterprise EHR configuration commonly runs for weeks, and through all of it someone has to take responsibility for the seams between three systems.
How to Improve Clinician Adoption of Ambient AI Scribes
Buying licenses and achieving adoption are separate accomplishments, and clinical software is full of tools that were purchased, shown once, and then used by a small minority of the people who could have used them. The difference tends to come down to a few human realities rather than to any feature on the comparison sheet.
Clinicians have to come to trust the note, which means the editing they do in the early weeks needs to leave the draft visibly better instead of feeling like the correction of a stranger’s work. The tool also has to suit the specialty, since a behavioral health session, a brisk orthopedic clinic, and a layered internal medicine visit pose genuinely different documentation problems, and a scribe that handles one of them well can frustrate another. And the benefit has to be framed accurately, which returns to the question of measurement. A physician told the tool will let them see more patients, will feel misled, whereas one told it will get them out of the building on time, and then showed their after-hours charting steadily falling, tends to become the kind of advocate whose enthusiasm carries down the corridor on its own.
The practices that make this work are unremarkable but decisive: a pilot run on real patient encounters instead of a scripted demonstration, a champion inside each department, a short feedback channel to the integration team through the opening month, and training that addresses the new habit of reviewing and signing rather than the mechanics of switching the tool on. None of that ships with the software, and all of it shapes whether the deployment takes hold.
How a Healthcare Integration Partner Supports Scribe Deployment
The scribe itself is a product, whereas the HIPAA-grade data governance, the EMR write-back, and the adoption work are projects, and those projects occupy the space between the vendor and the clinicians. That space is where a healthcare software and integration partner does its most useful work. Nalashaa operates on that layer for US health systems and HIT vendors, building BAA-aligned, secure data flows, dependable write-back into Epic and other EHRs through interfaces that have been tested against real workflows, and the operational structure that carries a three-month pilot into everyday clinical use.
What Determines the Success of an Ambient AI Scribe Deployment
The scribe is the smallest and simplest piece of this undertaking. The data governance that keeps patient audio compliant, the write-back that lands a clean note in the chart, and the change management that brings clinicians to depend on it are the substance of the work, and together they decide whether a health system ends up with fewer exhausted physicians or a contract gathering dust. Approached as an integration and adoption program rather than a procurement, the technology tends to deliver what the research has promised.
Nalashaa builds the secure integration and adoption layer that sits between ambient AI vendors, the EHR, and the clinicians who use it. Talk to our team about a scribe rollout that clinicians keep using.
Frequently asked questions
Are ambient AI scribes HIPAA compliant?
They can be, given the right implementation. The audio and the transcript are ePHI, so the deployment needs a Business Associate Agreement that covers the vendor’s AI processing, its retention practices, and any use of your data for training, alongside encryption in transit and at rest, defined access controls, and a human review step. Compliance depends on how you deploy and govern the tool rather than on any label the vendor applies.
Do you need patient consent to use an AI scribe?
HIPAA does not require special consent to document a treatment visit, but state recording laws sometimes do. In all-party-consent states, recording without informing the patient may breach wiretapping law, so a spoken disclosure, an updated Notice of Privacy Practices, and an option to decline have become standard practice.
Does an ambient AI scribe write directly into the EHR?
That depends on the integration. The deeper ones place the draft into the correct discrete chart fields, while lighter ones leave the clinician to copy and paste. Write-back depth, the retrieval of prior context, and the mapping to billing codes are the details that separate a tool clinicians keep from one they abandon.
Do AI scribes save clinicians time?
The more consistent benefit is a reduction in burnout and after-hours charting rather than a dramatic saving on each visit, which varies considerably by setting. Most studies find that visit length and patient throughput stay roughly constant, so the value lies in clinician wellbeing and in the quality of the documentation.
Who is responsible for errors in an AI-generated note?
The clinician remains responsible. An ambient scribe produces a draft and does not take responsibility for its contents, so the clinician who signs the note is accountable for its accuracy, which is why a review-and-edit step before the note enters the record is essential.
Latest posts by Priti Prabha (see all)
- Clinical Documentation Improvement: A Practical Guide - July 17, 2026