Telerehabilitation sits in an unusual spot among digital health categories. In most of them, the unsettled question is still whether the clinical benefit is real; in telerehabilitation, that argument has largely been won. Across musculoskeletal, cardiac, pulmonary, and vestibular rehabilitation, meta-analyses now report outcomes comparable to in-person care in pain, function, and patient satisfaction, whether the program runs through live video, through asynchronous exercise plans, or through remote monitoring. A 2025 perspective in the musculoskeletal literature framed the field’s remaining task as one of delivery rather than proof.
Those reframing matters, because the difficult decisions in a telerehabilitation program are rarely clinical ones. They concern which care model fits a given patient, how to deliver therapy over the uneven connections that real homes have, and how far the software is allowed to go before it stops being a support tool and becomes a regulated medical device. This piece works through those three questions, written for the health systems, clinics, and software teams putting telerehabilitation into the way they deliver care.
Choosing a care model that survives contact with the home
Telerehabilitation is usually described as three modes, and most programs end up blending them. Synchronous care is the live video session, the closest thing to an in-clinic visit and the right choice when a clinician needs to watch movement as it happens, correct form, or assess something new. Asynchronous care hands the patient a structured program of exercise videos, instructions, and a way to log progress or submit a clip for later review, and it carries most of the routine work of a rehabilitation course at a fraction of the scheduling and bandwidth cost. Remote monitoring adds wearables and sensors that report adherence and physiological signals between contacts, and in cardiac and pulmonary rehabilitation, it is frequently what makes home delivery safe enough to attempt at all.
The model is less than a single choice than a sequence. A knee replacement might open with a synchronous assessment, shift to an asynchronous program through the weeks of repetitive work and rely on monitoring to surface a patient who has quietly stopped progressing. Matching the mode to the condition, to the patient’s confidence with technology, and to the clinician’s need to see the patient is the design work that decides whether a program gets used or abandoned. Reimbursement belongs in that calculation from the beginning, since remote monitoring now has defined Medicare billing pathways that can fund the monitoring layer of a home program rather than leaving it as an unrecovered cost.
Designing Telerehabilitation for Low-Connectivity Environments
A telerehabilitation program is only as good as the link between the patient’s living room and the clinic, and that link is often the weakest part of the whole system. The FCC raised its benchmark for fixed broadband in 2024 to 100 Mbps down and 20 Mbps up, and a substantial share of rural America still falls short of it, while live video telehealth generally needs a steady 1.5 Mbps or more to be usable. A program designed only around a clean video call will fail exactly the patients who have the hardest time accessing in-person care.
Building around that reality changes the architecture. Asynchronous delivery is bandwidth-light by nature, because a stored exercise video or a submitted clip can travel across a slow connection over several minutes rather than demanding an uninterrupted real-time stream, which is why store-and-forward should usually carry the routine load while synchronous sessions are kept for the moments that clinically need them. The supporting measures are well-understood media that download progressively and play offline, an audio-only or telephone fallback for when video drops out, content sized for mobile data rather than home fiber, and reminders or check-ins that reach patients over SMS when they will never open an app. A national analysis of nearly eight million telemedicine sessions found broadband access and rurality to be stronger predictors of whether people use telehealth than social vulnerability on its own, which is a useful reminder that connectivity is the first barrier to clear without being the only one. Older patients and those with limited digital confidence need workflows that assume neither, and meeting them is a care-design problem as much as an engineering one.
When Telerehabilitation Software Becomes a Regulated Medical Device
The regulatory question runs underneath all of this and quietly sets the limits on what the software may do. In the United States, whether a piece of software counts as a regulated medical device turns not on the technology but on its intended use and the claims made for it. The 21st Century Cures Act amended the Food, Drug, and Cosmetic Act to remove from the device definition those software functions meant to maintain or encourage a healthy lifestyle that are unrelated to the diagnosis, treatment, mitigation, prevention, or cure of a disease, and the FDA’s General Wellness policy builds on that line by treating genuinely low-risk products that support healthy behavior as outside its active oversight.
A telerehabilitation tool that guides a clinician-prescribed exercise program, tracks adherence, and routes information back to a clinician who makes the clinical decisions generally sits in that lower-risk lane. The line is crossed once the software begins to do clinical work on its own, by diagnosing a condition, interpreting data to reach a clinical conclusion, or recommending or automatically adjusting treatment. At that point, the product meets the definition of software as a medical device and climbs the regulatory ladder, with the heavier evidence and quality obligations that come with the higher classes. Implied claims weigh as much as explicit ones, so positioning a general movement tool as something that treats a named condition can change its classification without a single line of code being touched.
For design, the consequence is to keep the clinician as the decision-maker and the software as the means of delivery and adherence, and to be deliberate about every claim attached to the product. The same logic holds in the European Union, where the Medical Device Regulation tends to push software that supplies information used for diagnostic or therapeutic decisions to at least Class IIa, leaving truly low-risk software in a narrow band. None of this argues against building capable tools. It argues for deciding early, with regulatory advice, which side of the line each feature belongs on, because reclassifying a product after launch costs far more than designing for the right class from the start.
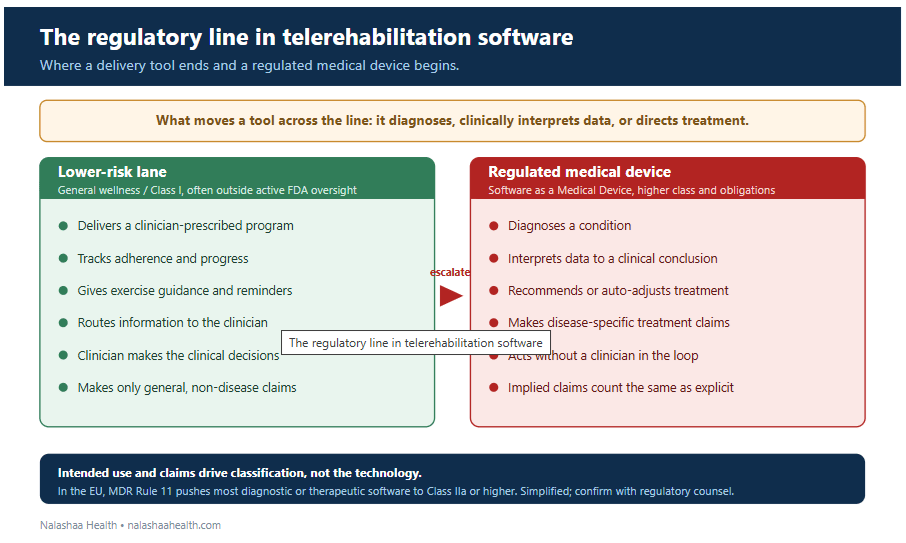
Figure: What keeps a telerehabilitation tool in the lower-risk lane, and the claims and functions that escalate it to a regulated medical device. Intended use and claims drive classification, not the underlying technology.
Technical and Operational Requirements for Telerehabilitation Software
Most of what decides whether a telerehabilitation program succeeds is therefore integration and design rather than rehabilitation science. It means connecting monitoring data and patient-reported progress back into the EHR and the clinician’s view, building the adherence and reminder mechanics that keep patients engaged across weeks of unsupervised work, supporting the spread of connections and devices that patients actually bring, and holding the product to the regulatory boundary it was designed for. Handled well, the technology delivers what the evidence has long promised, which is rehabilitation that reaches people who cannot easily reach a clinic.
What Determines the Success of a Telerehabilitation Program
The clinical case for telerehabilitation is settled. What decides whether a program reaches the people it is meant to help is the care model it offers, the range of connections it is built to tolerate, and the discipline to keep the software on the right side of the device line. The health systems and vendors that treat those three as design problems, rather than as afterthoughts, are the ones whose programs hold up once they leave the pilot.
Nalashaa builds remote care and rehabilitation software for US health systems and HIT vendors, from connectivity-resilient patient apps and monitoring integration to the clinician-facing tools that keep care coordinated. Talk to our team about home rehabilitation that works on the connections your patients actually have.
Frequently asked questions
What is telerehabilitation?
Telerehabilitation is the delivery of rehabilitation services, including physical, occupational, speech, cardiac, and pulmonary rehabilitation, to patients in their own homes through technology. It can run through live video, asynchronous exercise programs, remote monitoring, or a combination of the three.
Is telerehabilitation as effective as in-person care?
For many common conditions, the evidence is strong. Meta-analyses across musculoskeletal, cardiac, and pulmonary rehabilitation report outcomes comparable to in-person care in pain, function, and patient satisfaction. The remaining constraints tend to be practical, around connectivity, engagement, and how well a condition suits remote delivery, rather than clinical.
Is a telerehabilitation app a medical device that needs FDA clearance?
That depends on what the software does and how it is marketed. A tool that delivers a clinician-prescribed program and tracks adherence usually stays in the FDA’s low-risk or general wellness lane. If it diagnoses a condition, interprets data to reach a clinical conclusion, or recommends treatment, it can become software as a medical device and require the matching regulatory clearance.
How do you deliver telerehabilitation to patients with poor internet?
By leaning on asynchronous delivery, which needs far less bandwidth than live video, and by building in fallbacks such as offline-capable content, audio-only or telephone options, data-light media, and SMS reminders. Reserving live video for the moments that clinically require it keeps the program usable for patients on slow or unreliable connections.