What Does CMS Have to Say: 2023 Medicare Physician Fee Schedule
In 2019, a terrible pandemic swept across the world. A pandemic that forced us to stay at home but also increased our dependency on doctors. Keeping this in mind, the US govt decided to add multiple new temporary CPT and HCPCS codes to the telehealth reimbursement model. Providers could now offer services without worrying about reimbursements. This year we are witnessing the pandemic slowly wilt away and the worldly cogs have again started to move at their regular pace.
Consequently, on July 2022, CMS released its proposed 2023 Medicare physician fee schedule. This has proposed substantial changes for the post-pandemic reimbursement module.
A Sneak-peak into the Proposed Reforms
-
Proposal to add three new telehealth codes for prolonged E/M services
- GXXX1(Prolonged hospital inpatient or observation care evaluation and management service(s) beyond the total time for the primary service (when the primary service has been selected using time on the date of the primary service); each additional 15 minutes by the physician or qualified healthcare professional, with or without direct patient contact (list separately in addition to CPT codes 99223, 99233, and 99236 for hospital inpatient or observation care evaluation and management services).
- GXXX2 (Prolonged nursing facility evaluation and management service(s) beyond the total time for the primary service (when the primary service has been selected using time on the date of the primary service); each additional 15 minutes by the physician or qualified healthcare professional, with or without direct patient contact (list separately in addition to CPT codes 99306, 99310 for nursing facility evaluation and management services).
- GXXX3 (Prolonged home or residence evaluation and management service(s) (Prolonged home or residence evaluation and management service(s) beyond the total time for the primary service (when the primary service has been selected using time on the date of the primary service); each additional 15 minutes by the physician or qualified healthcare professional, with or without direct patient contact (list separately in addition to CPT codes 99345, 99350 for home or residence evaluation and management services).
-
Proposal to Add 54 codes to the category 3 list:
The category 3 list of CMS contains services that lack proper evidence to justify permanent coverage. In the 2023 Medicare Physician fee schedule (PFS), CMS proposed adding 54 codes to this list. The services of these codes broadly fall under these nine categories. (1) audiology; (2) ophthalmologic; (3) behavioral health; (4) adaptive behavior treatment and behavior identification assessment; (5) electronic analysis of implanted neurostimulator pulse generator/transmitter ; (6) speech therapy; (7) cognition; (8) ventilator management; and (9) therapy. To check the entire list click on this link. All the category 3 codes were set to expire at the end of the year in which the Public Health Emergency (PHI) ends but CMS has now extended their coverage till 31st December 2023.
-
Reimbursement for telephone (Audio-only) E/M services to be discontinued
- During the PHE, CMS had allowed the telephone (Audio/only) E/M services for separate reimbursement. This was utilized extensively by both providers and patients, especially by patients without proper network bandwidth for audio-visual interactions.
- CMS has decided not to permanently add these to the Medicare Telehealth Services List but it has also made an exception for certain telemental health services.
- The Section 1834(m)(2)(A) of the Social Security Act states that telehealth services are to be considered only when they can serve as an alternative for a face-to-face encounter.
- The proposed PFS states that CPT codes 99441-99443 are to be discontinued from the Medicare Telehealth Services List. Consequently, providers will not receive any separate reimbursement for these services. They will be covered by the pre-PHE bundle status under Medicare.
- This change will take place 151 days after the PHE expires.
-
Virtual Direct Supervision is to be discontinued
- During the Public Health Emergency, CMS temporarily changed the direct supervision rules. This means that the supervising professional and the patient can be present in two different locations during the encounter. As a consequence of the PHE interactions through real-time, interactive audio-visual technology was necessary and therefore allowed.
- CMS now feels that such direct supervision via virtual presence might not be safe for all kinds of clinical emergencies.
- The supervision waiver will expire at the end of the year on which the PHE ends. This also depends on the date by which the proposed rule gets finalized.
-
Reimbursement for telephone (Audio-only) E/M services to be discontinued
- During the PHE, CMS had allowed the telephone (Audio/only) E/M services for separate reimbursement. This was utilized extensively by both providers and patients, especially by patients without proper network bandwidth for audio-visual interactions.
- CMS has decided not to permanently add these to the Medicare Telehealth Services List but it has also made an exception for certain telemental health services.
- The Section 1834(m)(2)(A) of the Social Security Act states that telehealth services are to be considered only when they can serve as an alternative to a face-to-face encounter.
- The proposed PFS states that CPT codes 99441-99443 are to be discontinued from the Medicare Telehealth Services List. Consequently, providers will not receive any separate reimbursement for these services. They will be covered by the pre-PHE bundle status under Medicare.
- This change will take place 151 days after the PHE expires.
-
Virtual Direct Supervision is to be discontinued
- During the Public Health Emergency, CMS had temporarily changed the direct supervision rules. This means that the supervising professional and the patient can be present in two different locations during the encounter. As a consequence of the PHE interactions through real-time, interactive audio-visual technology was necessary and therefore allowed.
- CMS now feels that such direct supervision via virtual presence might not be safe for all kinds of clinical emergencies.
- The supervision waiver will expire at the end of the year on which the PHE ends. This also depends on the date by which the proposed rule gets finalized.
Overview of Telemental Six-month Rule from Congress
The congress in 2020 released new conditions for telemental health coverage under Medicare. A telemental health service will only be covered under Medicare if it fulfills the following conditions.
- The practitioner conducts an in-person exam of the patient within six months before the initial telehealth service;
- The telehealth service is furnished for purposes of diagnosis, evaluation, or treatment of a mental health disorder (other than for treatment of a diagnosed substance use disorder (SUD) or co-occurring mental health disorder); and
- The practitioner conducts at least one in-person service every 12 months of each follow-up telehealth service.
These are to take effect 151 days after PHE ends.
A Glimpse of the Future from Collected Data
The last decade has proved how fast technology is evolving. We have moved from Megabytes to Terabytes and finally have touched new horizons with cloud engineering. Today over 5 billion of us are on the internet. And that number is only going to increase. Thus, it is quite natural to assume that the use cases of telehealth will also expand in the coming years. Well, let’s not assume, let’s see what the data suggests.
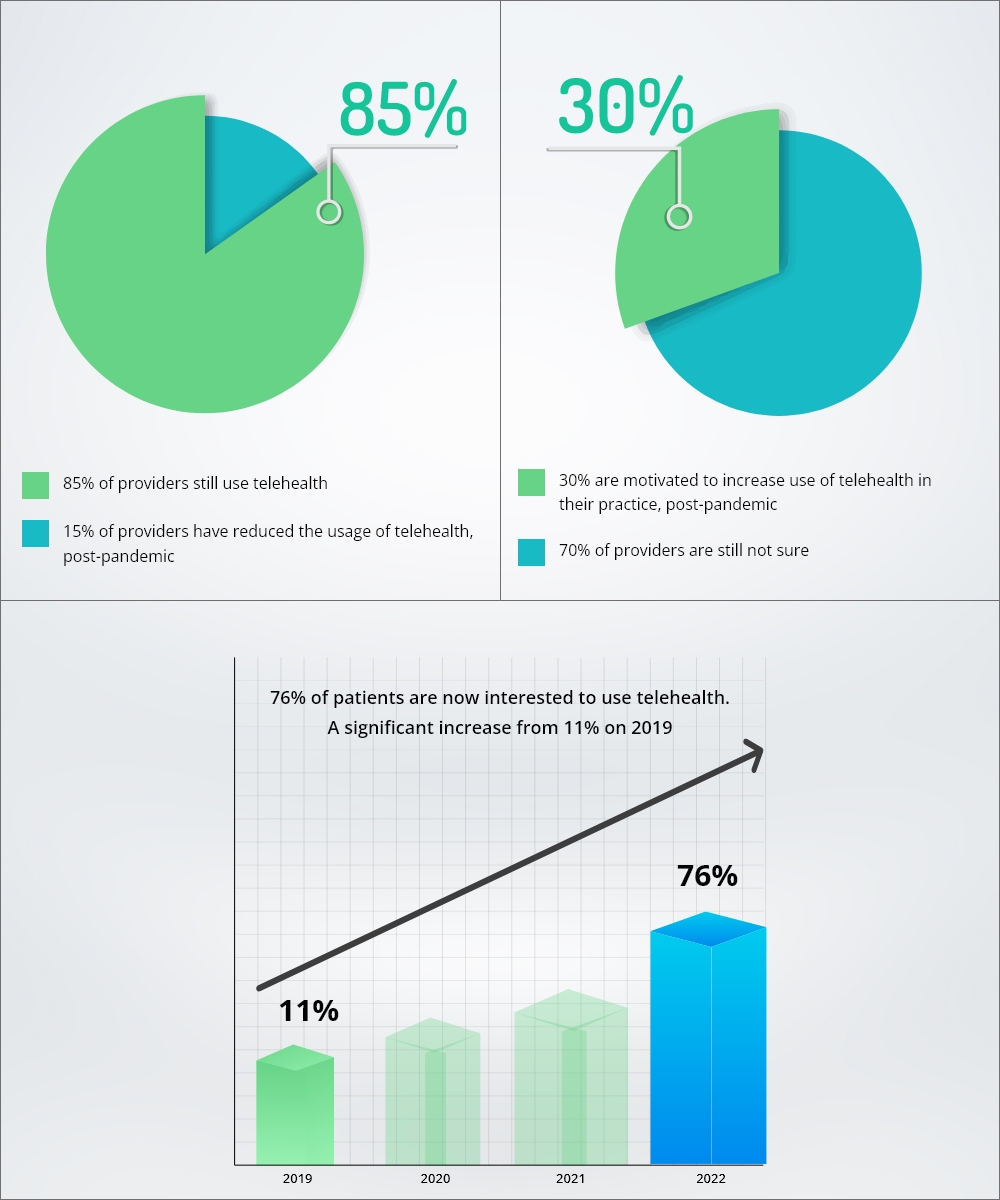
Taken from a survey from AMA and mckinsey
What are the Technical Implications of the Proposed Reforms
Although this is a proposed rule, a version of it with minor to no changes will come out by the end of this year. The proposed rules suggest only one thing. Telehealth is soon going to become a norm and the Government is just trying to make sure that it grows properly.
We understand that changes are never easy. But if implemented correctly they can feel like a soothing mountain breeze rather than a hurricane.
Provider Solutions In a Nutshell:
- Compliance: Rules and regulations are full of complicated jargon. But you also can’t ignore them due to the high penalties for noncompliance. Get help from a compliance expert. They will help you comprehend the rules and also make your system compliant.
- Upgradation: New Rules usually suggest that the technology will now be regulated but also regularly used. Every technology that is commonly used comes with regular upgrades. Your system needs to be updated to absorb all these changes to telehealth.
- EHR Customization: As a provider, your main focus should be value-based patient care and not data management. An integrated and customized EHR can free you from such mundane tasks. No longer will you have to visit different portals to update patient information.
- Smart Applications: From smartphones to smart refrigerators, we have come a long way. So, why settle for a poorly made application? Smart telehealth applications can detect non-reimbursable encounters before scheduling, provide you with patient alerts, automatically record patient data, and much more. It is just like an assistant but doesn’t bill you at end of the month.
- Revenue Cycle Management: A robust and upgraded RCM solution coupled with intelligent automation means fewer roadblocks during reimbursement.
- Data security: Securing messaging with end-to-end encryption is of paramount importance. Standardized data transfer with the help of Govt. approved APIs is needed, too. These are just a glimpse of what you can do for data security.
Conclusion
The solutions above are usually beyond the scope of an IT department in a provider network. However, the only way to survive is to evolve. You can ease this voyage over the tides with the help of an experienced healthcare solution partner.
That is where we come in. For more than ten years, Nalashaa has been a one-stop shop for all things healthcare solutions. Check out our plethora of Healthcare provider solutions that have been enhancing provider networks across the USA.
Or Connect with us at info@nalashaa.com.
Mitrajit Das
Latest posts by Mitrajit Das (see all)
- Revolutionizing Healthcare Communication: The AIDET Approach - March 17, 2025